ANSIRH is working collaboratively with the Center for Public Health Law Research at Temple University and Penn State College of Medicine to investigate relationships between state-level abortion policies and adverse maternal and child health (MCH) outcomes and which subgroups these policies affect most. This study will be the first of our knowledge to use rigorously coded, longitudinal policy data to answer key questions about the population-level impact of abortion policies, including questions about differences between adopted policies versus those that are in effect and the extent to which policy severity (i.e. length of waiting period, parental notification vs. parental consent, etc.) matters.
Research Aims
Study Design
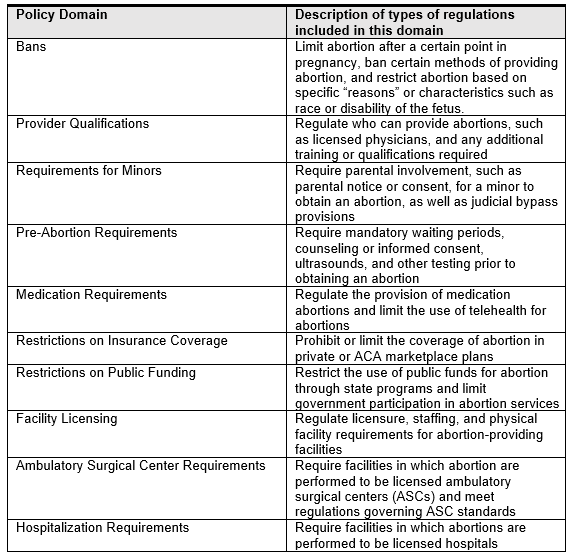
In this study, our Temple collaborators will be precisely classifying which abortion policies exist in each U.S. state from 2005-present. The ANSIRH team will then use epidemiologic and econometric methodologies to examine relationships between these policies and MCH outcomes (e.g. birthweight, maternal morbidities, and infant and maternal mortality) and explore possible mechanisms through which policies relate to these outcomes (e.g. through changes in numbers of abortions/births, changes in intendedness of births, stress among people who give birth). We will examine a wide range of abortion polices – including post-Dobbs abortion bans – as outlined in the table below.
At the end of the project (in 2027/2028), policy data will be made publicly available. Researchers interested in using these policy data for research purposes before then and who have a research question that is outside the domain of the planned work should contact the PI (Dr. Sarah Roberts). Prior to the end of the project, decisions about use of the data for these purposes will be made on a case-by-case basis.
Data on MCH outcomes will be obtained from public and private insurance claims data, Vital Statistics data, and Pregnancy Risk Assessment Monitoring System (PRAMS) survey data.
Implications
The rise in restrictive abortion policies, particularly since the Dobbs vs. Jackson Women’s Health Supreme Court Decision that removed protections for legal abortion in U.S. states, is predicted to decrease people’s ability to obtain abortions and thus increase the number of people who give birth after becoming pregnant. As more people continue their pregnancies and give birth, it is important to understand how restricting abortion affects the health and wellbeing of birthing people and their infants, which groups are most affected by these policy changes, and whether any other state-level policies (e.g. expanded Medicaid; structural racism policies) may mitigate or exacerbate any adverse health effects.
The findings produced by this study will provide key evidence to policymakers seeking to improve health and well-being of pregnant and birthing people and their children. Understanding whether and to what extent the high rates of adverse MCH outcomes in the U.S. are due, in part, to abortion policies; under what conditions adverse effects occur; and for which populations adverse effects occur is essential for mitigating adverse health effects of policies. This is of particular important in informing program planning for health departments and other health professionals responsible for serving and caring for people unable to obtain abortions and their children.
We anticipate that the first findings will be available beginning sometime in 2025.
The research referenced on this page is supported by the U.S. National Institute of Child Health & Human Development at the National Institutes of Health [Grant R01HD108337]. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or other funders.