Growing barriers to abortion care in the United States have increased interest in self-managed abortion, defined as attempting to end one's own pregnancy without clinical supervision. ANSIRH researchers aimed to assess association of attempted self-managed abortion with reported barriers to abortion care. This infographic summarizes what they found.
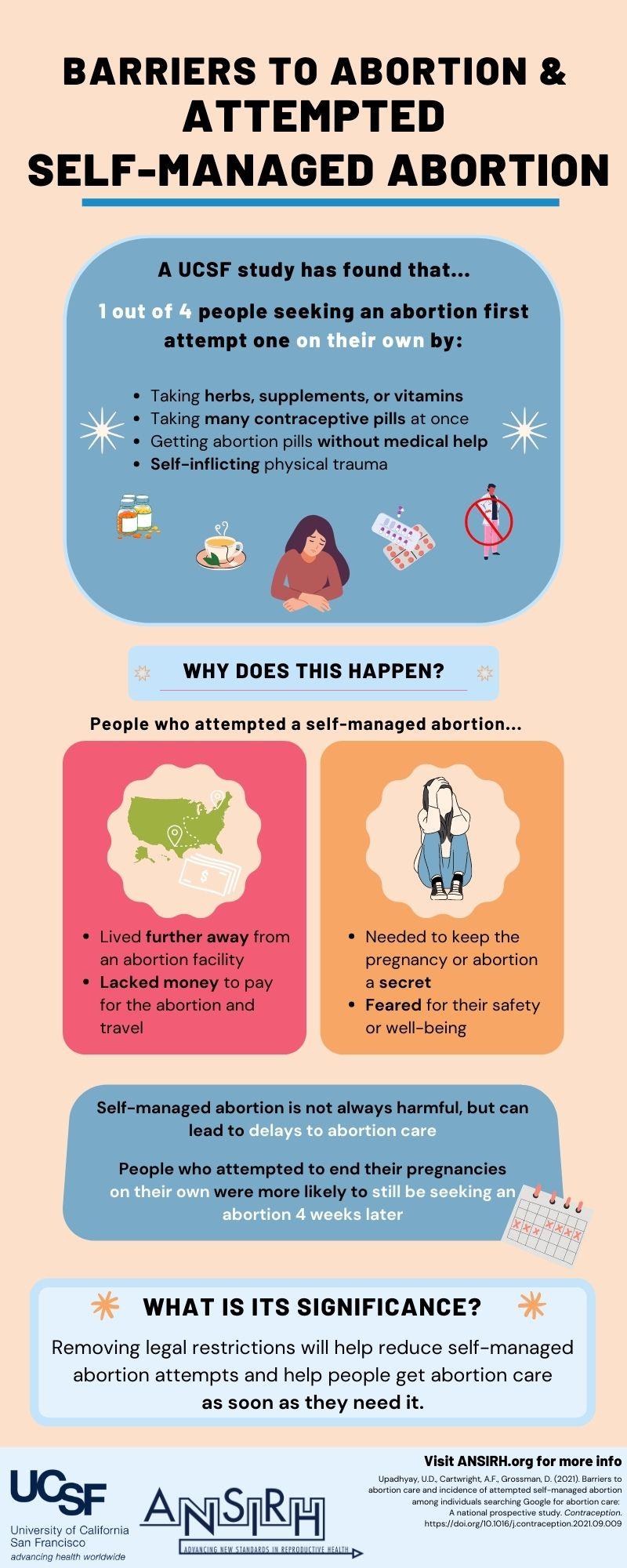
Using data from the Google Ads Abortion Access Study, researchers found that participants reported a broad range of methods used to self-manage their abortions, some of which have not previously been captured in the literature. Most common methods used were: herbs, supplements, or vitamins (52%); emergency contraception or many contraceptive pills (19%); mifepristone and/or misoprostol (18%); and abdominal or other physical trauma (18%). Reporting having to keep the abortion a secret, fearing for one's safety/well-being, needing to gather money for travel or the abortion, or living further from an abortion facility as barriers were associated with higher odds of attempts.
The researchers conclude that people who experienced these obstacles were more likely to attempt self-managed abortion, which can lead to delays in accessing medical care if it is unsuccessful. The results demonstrate the need to remove legal restrictions on abortion as a first step to reduce barriers to abortion. Additionally, innovative methods to expand equitable access are essential, including increasing the number/types of clinicians who can provide abortion, allowing pharmacy access to abortion pills, and approving telehealth models of abortion care, all of which would likely reduce attempted self-managed abortion.
Barriers to abortion care and incidence of attempted self-managed abortion among individuals searching Google for abortion care: A national prospective study can be found in Contraception.