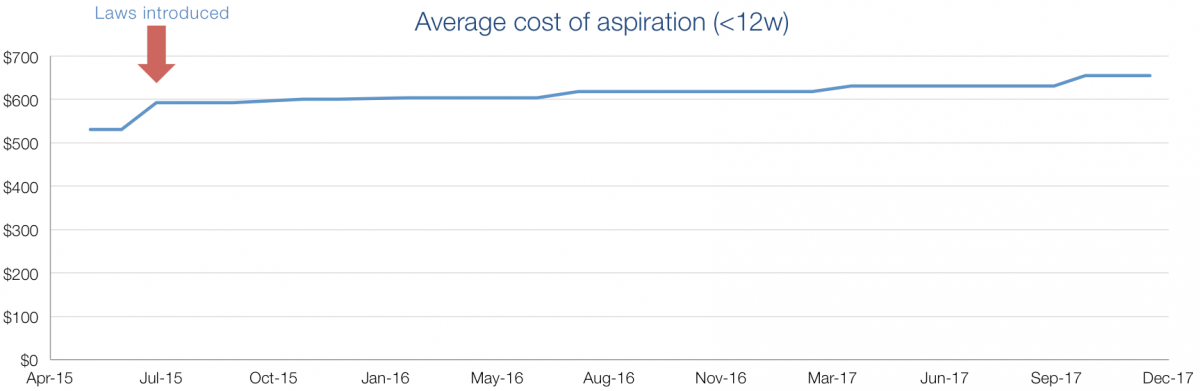
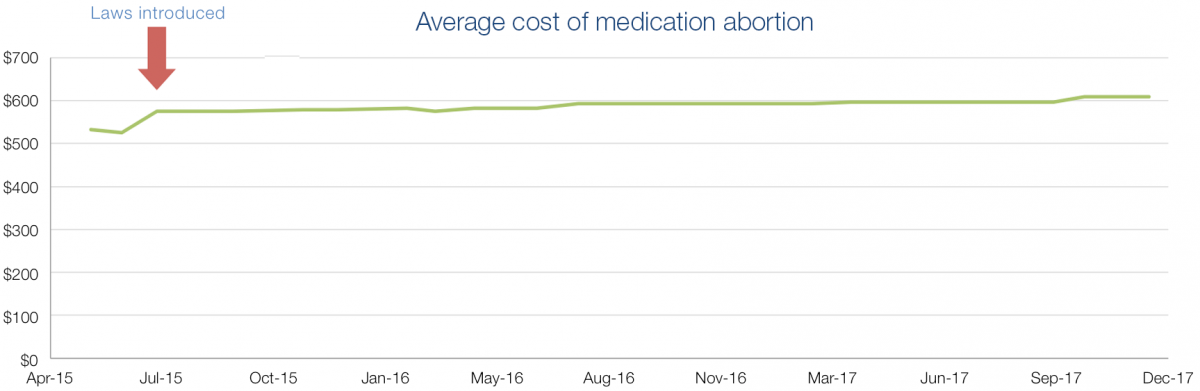
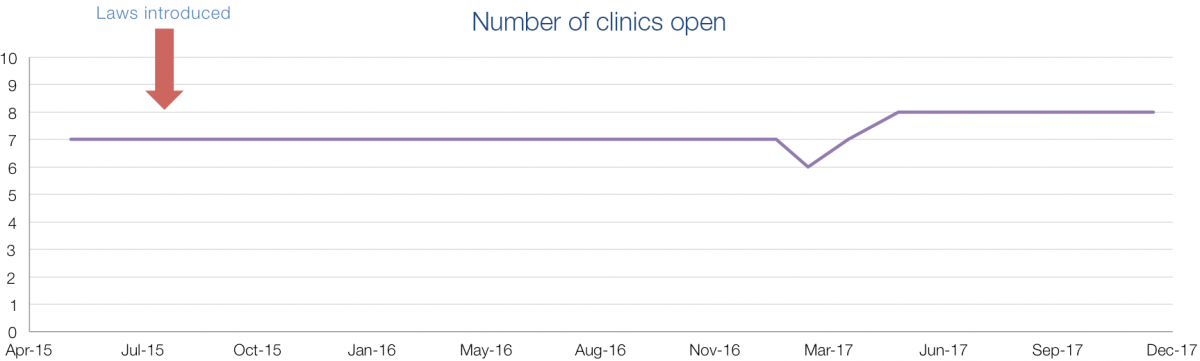
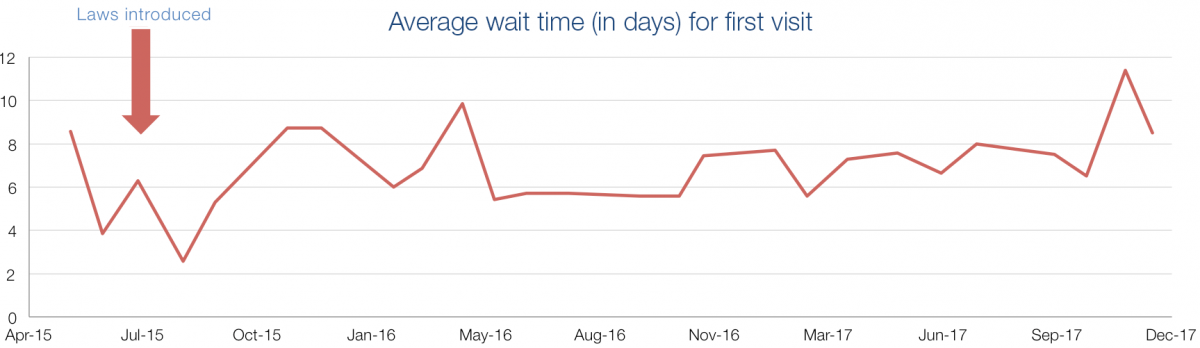
In July 2015, changes to the Tennessee constitution (Amendment 1) opened the door for abortion restrictions that had previously been prohibited. On July 1, 2015, the state enacted a mandated information requirement and a 48-hour waiting period, resulting in a two-visit requirement. A law requiring that all abortion providers conducting 50+ abortions per year be licensed as ambulatory surgical treatment centers was also enacted at the same time, but is permanently enjoined and not in effect.
By studying Tennessee as abortion becomes increasingly restricted, we aim to understand the cumulative effect of many restrictions on women’s access and experiences with abortion.
Key Findings
- back to the Evaluation of Abortion Restrictions Project
Study Design
To understand the cumulative impact over time of several new abortion restrictions on women’s access to abortion care in Tennessee, research staff made monthly mystery telephone calls to all abortion providing clinics in the state to collect real-time data on services offered (medication abortion, aspiration abortion, gestation limits for each), costs of abortion, number of days to first available appointment, and visit logistics (e.g., waiting period, two-visit requirement). Monthly calls were made for 2½ years.
Implications
Because these data were collected at the clinic level, these findings cannot support conclusions about the experiences of individual patients. Further research is needed among patients to understand how these laws impacted patient costs for the abortion, as well as travel, childcare, and other costs.
Increased wait times may be masked by counseling visit requirements. We were not able to collect data on time until the day of the abortion, but given that average wait time to the counseling appointment stayed near constant, time until abortion has increased by at least 2 days since the introduction of the 48-hour waiting period requirement.
These data cannot lead to conclusions about the individual wait times to the abortion appointment. Research is needed among individual patients to better understand the effects of the law on waiting time until patients can have an abortion which may be a more useful indicator of patient experience.